Introduction
Migraine is a debilitating condition, representing the second leading cause of disability globally. In a recent epidemiological study in the United States, 19.2% of individuals have self-reported a migraine, with 15.8% reporting at least one monthly headache day over 3 months. Of the 18,353 respondents who met the criteria for migraine, migraine disproportionately affected women versus men. Of the 15,133 (women; n = 11,049, men; n = 4084) reporting at least one migraine headache day per month, the ratio of women to men with migraine was 3:1. Overall, 18% of American women and 6% of men experience migraine headaches.
It is estimated that more than 90% of individuals use medication for the acute treatment of their migraine headaches. However, approximately 36% of those who use medication for their headaches discontinue treatment, and lack of treatment efficacy ranks among the top reasons for suspending treatment. While numerous administration routes for acute therapy for migraine exist, oral tablets are the most commonly prescribed for patients. However, bio-availability or the rate and extent to which a drug reaches the systemic circulation, becomes a challenge with oral administration because oral drugs must first pass through the stomach and into the small intestine of the gastrointestinal (GI) system before they can be absorbed. Bioavailability is subject to variations in intestinal absorption, and in addition, even well-absorbed drugs may then undergo high rates of hepatic first-pass metabolism, which may make them pharmacologically inactive. Additionally, disparities in gut motility and metabolism among individuals, and even within an individual on different occasions, may affect bioavailability.
The oral medications may not be ideal for migraine patients experiencing gastroparesis, as delayed absorption may cause migraine symptoms to worsen. Migraine commonly accompanied by nausea may lead to reluctance to take oral treatment, and vomiting may lead to ingested drugs being lost in vomitus and uncertainty about whether to re-dose.
Migraine and disorders of the nose can be comorbid conditions, which suggests a possible underlying pathophysiological relationship. Rhinitis is a comorbidity of migraine, and epidemiological studies have shown that a relationship between rhinitis and migraine exists. A 2008 questionnaire study demonstrated that the frequency of migraine attacks is significantly increased in patients with rhinitis and that rhinitis is associated with increased headache disability. Another study demonstrated that migraine was substantially more prevalent in patients with rhiniti and that the odds of experiencing a migraine attack were 14.3 times higher in patients with rhinitis. Additionally, unilateral cranial autonomic symptoms, which include nasal congestion and rhinorrhea, can occur during a migraine attack. A 2006 study revealed that migraine patients with UASs experienced longer migraine duration, increased head pain severity, and more frequent allodynia and photophobia compared to migraine patients without UASs. Olfactory triggers are common in those with migraine, occurring in 90% of migraine patients in a 2016 study. In those patients who experienced odor-triggered migraine attacks, osmophobia was reported by 95% of patients. Additionally, reduced olfactory acuity was reported by patients who underwent osmophobia and odor-triggered headaches. Such evidence underpins a connection between the nose and migraine, and thus a nasal treatment may make more logical sense than previously appreciated.
Nasal delivery has promised to be an effective alternative route of administration for over 25 years. Yet, despite many effective migraine drugs being formulated for nasal administration, they have failed to generate consistent or convincing efficacy data for all patients with migraine attacks, and most have not been commercially successful. This review will discuss the shortcomings of approved nasally delivered therapies and the current attempts to overcome the issues associated with traditional nasal delivery of acute medications for migraine. The nose is a complex organ, and the need to deliver efficacious medication to the appropriate anatomical region of the nose may have been underestimated.
Nasal sprays have become a valuable and convenient mode of administering medication for the acute treatment of migraines. They offer several advantages over traditional oral medications, especially regarding rapid relief. Migraines are neurological disorders characterized by severe and often debilitating headaches that can be accompanied by additional symptoms like nausea, vomiting, light sensitivity (photophobia), and sound sensitivity (phonophobia). The key to effective migraine treatment is early intervention to alleviate symptoms and prevent the progression of the headache.
Nasal Sprays for Migraine
The nasal sprays for migraine treatment are pharmaceutical formulations designed to be administered through the nostrils. They are primarily used to deliver medications directly to the bloodstream through the nasal mucosa, bypassing the digestive system and liver, which can delay the onset of relief when using oral medications. Nasal sprays are favored for migraine treatment because they offer rapid absorption of the active medication. The mucous membranes lining the nasal passages have a rich blood supply, which allows for quick absorption and distribution of the medication throughout the body. This rapid onset of action can be particularly beneficial during a migraine attack when timely relief is essential.
Triptans are a class of medications commonly used for migraine treatment. Triptan nasal sprays contain these active ingredients, such as sumatriptan and zolmitriptan. They work by constricting blood vessels in the brain and blocking pain pathways, effectively relieving migraine symptoms.
DHE Nasal Sprays: Dihydroergotamine (DHE) is another medication available in nasal spray form for migraine treatment. DHE nasal sprays work by constricting blood vessels and reducing inflammation in the brain, offering relief from migraine symptoms.
Advantages of Nasal Sprays over Oral Medications for Acute Migraine Treatment
Nasal sprays provide an alternative route of administration for individuals who may have difficulty swallowing or keeping oral medications down during a migraine attack. They can provide faster relief compared to some oral medications, making them especially useful for migraines with rapid onset and severe pain. Nasal sprays may reduce the risk of gastrointestinal side effects, such as nausea and vomiting, which are common during migraines.
Other advantages include at-home administration, non-invasiveness, easy self-administration, and avoidance of drug degradation in the G.I. tract and first-pass metabolism (similar to injection), which allows for enhanced bioavailability and reduction of systemic side effects without the use of a needle.
Proper administration of nasal sprays is crucial for their effectiveness. Patients should carefully follow the instructions provided with the specific medication. This typically involves inserting the nozzle of the spray into one nostril, activating the spray, and inhaling the medication while keeping the other nostril closed. The process may need to be repeated for the second nostril.
One of the main benefits of a migraine nasal spray is how quickly it takes effect. A single spray of a triptan nasal spray can provide relief in as little as 15 minutes, compared to about 30 minutes for an oral medication. While an injection can take effect within minutes, a nasal spray can be easier and less invasive to administer.
Mechanism of Nasal Spray
Nasal sprays for migraine can offer more rapid relief than oral medications. In fact, a 2013 research review showed that it's possible for nasal sprays to begin to ease the symptoms of an acute migraine attack in as quickly as 15 minutes. Generally speaking, medications that are given intranasally can be absorbed more rapidly and effectively than oral medications.
The nasal cavity contains a high amount of blood vessels. This provides a more direct route for the drug into your bloodstream. When a drug is directly absorbed into your bloodstream, it avoids being broken down by your digestive system or the liver during first-pass metabolism. This means more drug is readily available to counteract your migraine symptoms.
Below are the general mechanisms behind the drugs that are used in migraine nasal sprays:
Triptans are one of the first-line treatments for migraine that's moderate-to-severe in intensity. The doctor may recommend a triptan if using NSAIDs or acetaminophen is ineffective for easing acute migraine symptoms. These drugs bind to certain subtypes of brain receptors specific for serotonin. Serotonin is a neurotransmitter whose levels are important in migraine.
When a triptan binds to these receptors, it causes blood vessels in your brain to tighten (vasoconstriction). This has the effect of lowering pain signaling and inflammation.
Mechanism of Action
Three distinct mechanisms of action of triptans have been described in migraine:
Vascular mechanism: Vasoconstriction of painfully distended intracranial extracerebral arteries directly affects vascular smooth muscle.
Trigeminovascular mechanism: Inhibition of nociceptive neurotransmission within the trigeminal nerve in the brainstem and upper spinal cord.
Central mechanism: Inhibition of vasoactive neuropeptides by trigeminal nerve innervating the intracranial vessels and dura mater.
Triptans act as antimigraine agents by selectively binding to the serotonin receptors 5-HT1B and 5-HT1D. Triptan binding to the vascular 5-HT1B receptors leads to vasoconstriction of the cranial arteries, which painfully dilate during a migraine attack. When triptans bind to the neurogenic and central 5-HT1D receptors, they prevent the release of vasoactive neuropeptides by inhibiting trigeminal nerves' activation and blocking the transmission of pain signals to the brain.
Generally speaking, triptans have replaced ergotamines as one of the primary treatments for acute migraine attacks. The doctor may prescribe ergotamine if other medications haven't relieved the symptoms effectively. Ergotamines also bind to serotonin receptors in your brain. This causes blood vessels to constrict and lowers pain signaling. However, they're also less specific than triptans, which can cause more side effects.
NSAIDs inhibit an enzyme called cyclooxygenase (COX) 1 and 2, which block the production of prostaglandins. Prostaglandins are chemicals that are important in contributing to pain and inflammation.
Ketorolac, the type of NSAID available as a nasal spray, can be prescribed to help with migraines that cause severe pain.
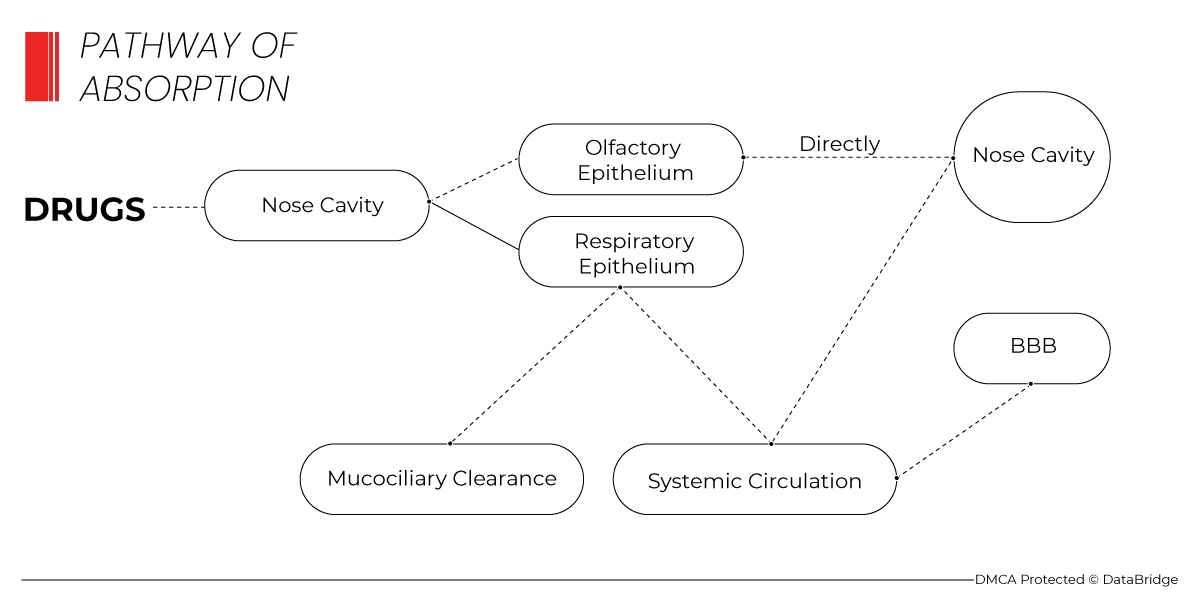
1 Pathway of Absorption
Comparator Studies between Nasal Routes of Delivery and Oral Tablets
Studies have suggested that nasal delivery of some triptans provides a more rapid onset with greater efficacy than oral triptan tablets. The COMPASS study was a randomized, active-comparator, double-dummy, crossover, multi-attack study that compared the efficacy, tolerability, and safety of breath-powered nasal delivery containing a low dose (22 mg, AVP-825 (ONZETRA Xsail)) of sumatriptan versus oral delivery (100 mg) of sumatriptan. Results showed that ONZETRA plus placebo pill (ONZETRA) significantly reduced migraine pain intensity compared to 100 mg oral sumatriptan plus placebo nasal product (oral sumatriptan) in the first 30 minutes post-dose.
It was postulated that early rates of pain relief might reflect quick systemic absorption of the sumatriptan powder delivered to the highly absorptive upper nasal cavity via the breath-powered device. Rates of pain relief and freedom at two h and sustained pain freedom from 2 to 48 h for ONZETRA were comparable to oral sumatriptan.
Overview of Approved Nasal Products
Several nasal products are currently approved for the acute treatment of migraine. While nasal powder formulations exist, the nasal drug market is currently dominated by liquid formulations.
IMITREX (GlaxoSmithKline) was approved in the U.S. in 1997 as a nasal spray. It delivers sumatriptan, a serotonin receptor agonist, via a standard nasal spray and is indicated for the acute treatment of migraine with or without aura. The recommended adult dose is 5, 10, or 20 mg, with 5 and 20 mg doses administered in a single spray and 10 mg in two sprays.
Each 100 µL spray of IMITREX contains 5 or 20 mg sumatriptan in an aqueous buffered solution containing monobasic potassium phosphate National Formulary (N.F.), anhydrous dibasic sodium phosphate United States Pharmacopeia (USP), sulfuric acid N.F., sodium hydroxide N.F., and purified water USP. The solution's pH is approximately 5.5, with an osmolality of 372 or 742 mOsmol for the 5 and 20 mg doses.
MIGRANAL (Bausch Health Companies Inc.) received U.S. approval in 1997 and is a dihydroergotamine (DHE) mesylate nasal spray indicated for the acute treatment of migraine with or without aura. It utilizes a traditional nasal delivery system that targets DHE mesylate to the lower nasal space. In addition to DHE mesylate, each dose contains anhydrous caffeine, anhydrous dextrose, carbon dioxide, and purified water and its pH is approximately 4.4–5.4 in solution
MIGRANAL acts by binding to serotonergic, dopaminergic, and adrenergic receptors. The recommended dosing is a single 0.5 mg/mL spray administered in each nostril, followed by one additional spray in each nostril 15 min later, for a total of 2 mg MIGRANAL delivered in four sprays.
ZOMIG (Amneal Pharmaceuticals) was approved in 2003 in the U.S. It is a zolmitriptan-containing nasal spray indicated for the acute treatment of migraine with or without aura that has been shown to deliver zolmitriptan to the nasopharynx and lower nasal space. It is a serotonin receptor agonist with a recommended starting dose of 2.5 mg; however, 5 mg can be used if headache relief is not achieved with 2.5 mg. Each 100 µL dose is supplied in an aqueous buffered solution containing anhydrous citric acid, disodium phosphate dodecahydrate USP, and purified water USP in addition to 2.5 or 5 mg of zolmitriptan buffered to pH 5.0. The solution is hypertonic, and its osmolarity is 360 to 420 and 420 to 470 mOsmol for the 2.5 and 5 mg dose, respectively.
ONZETRA Xsail (Currax Pharmaceuticals LLC) received U.S. approval in 2016. It is a sumatriptan nasal powder contained in a disposable, single-use nosepiece containing 11 mg sumatriptan base in a clear hypromellose capsule attached to a reusable delivery device body containing a mouthpiece and piercing mechanism. It is delivered into the nostril by blowing through the mouthpiece while the nosepiece is inserted into one nostril. The recommended dosing is achieved by delivering the contents of one 11 mg nosepiece to each nostril for a total of 22 mg.
TOSYMRA (Upsher-Smith Laboratories) was approved in 2019 in the U.S. and is a nasal spray containing sumatriptan, and a permeation-enhancing excipient (0.2% 1-O-n-Dodecyl-β-d-maltopyranoside (DDM, Intraveil®)) indicated for the acute treatment of migraine with or without aura. Its site of drug deposition within the nasal cavity has not been explicitly stated in the literature. However, the inclusion of the permeation-enhancing excipient, DDM, can enhance the absorption and bioavailability of drugs delivered intranasally. In addition to sumatriptan and DDM, each 100 µL dose is supplied in an aqueous buffered solution containing citric acid monohydrate, potassium phosphate monobasic, sodium chloride, and anhydrous sodium phosphate dibasic. Its pH is approximately 5.0–6.0, and its osmolality is between 270 and 330 mOsmol.
Products in Development
A nasal DHE powder delivered from a disposable nasal delivery device (STS101) is currently in development by Satsuma Pharmaceuticals (South San Francisco, CA, USA). A Phase 1, randomized, open-label, safety, tolerability, and comparative bioavailability study of STS101 demonstrated quick systemic absorption, attaining effective DHE plasma concentrations (>1000 pg/mL) within 10 min.
Although the pharmacokinetics of STS101 demonstrated values that were 2.3-fold higher than those of MIGRANAL, it utilized a 6 mg dose that was 300% of the approved MIGRANAL 2 mg dose. The results of topline data from the EMERGE trial, a Phase 3, multicenter, single-dose, randomized, double-blind, placebo-controlled, parallel-group efficacy study, showed that although numerical differences were in favor of STS101, the study did not demonstrate statistically significant differences between dosage strengths (4 and 6 mg) compared to placebo on coprimary endpoints of pain and most bothersome symptom freedom (among photophobia, phonophobia, or nausea) at 2 h post-administration.
Impel NeuroPharma (Seattle, WA, USA) currently has a novel drug–device combination product in development (and submitted a new drug application (NDA) in November 2020) that targets delivery of liquid DHE mesylate to the upper nasal cavity using a Precision Olfactory Delivery (POD) device (INP104). The POD technology has been developed to address the low bioavailability and variability in nasal administration seen with traditional nasal sprays. The drug delivery of INP104 to the upper nasal space takes advantage of the olfactory region's abundant vascularity and avoids drug loss due to the drug dripping out of the nose or clearance to the nasopharynx, thereby increasing systemic availability.
Data Bridge Market Research analyzes that the global nasal spray market is expected to reach a value of USD 38,026.75 million by 2030, at a CAGR of 6.7% during the forecast period. In 2023, North America is dominate the global nasal spray market due to the increasing investment in nasal spray, which is expected to boost the market growth. The U.S. is dominating the North America nasal spray market due to the strong presence of key players.
To know more about the study, visit: https://www.databridgemarketresearch.com/reports/global-nasal-spray-market
Data Bridge Market Research analyses that the nasal drug delivery technology market was valued at USD 64.2 billion in 2021 and is further estimated to reach USD 110.31 billion by 2029, and is likely to grow at a CAGR of 7% during the forecast period of 2022 to 2029. The market report curated by the Data Bridge Market Research team includes in-depth expert analysis, patient epidemiology, pipeline analysis, pricing analysis, and regulatory framework.
To know more about the study, visit: https://www.databridgemarketresearch.com/reports/global-nasal-drug-delivery-technology-market
Recent Developments
Pfizer's ZAVZPRET™ (zavegepant) Migraine Nasal Spray Receives FDA Approval
In March 2023, Pfizer Inc. announced that the U.S. Food and Drug Administration (FDA) had approved ZAVZPRET™ (zavegepant), the first and only calcitonin gene-related peptide (CGRP) receptor antagonist nasal spray for the acute treatment of migraine with or without aura in adults.
In its pivotal Phase 3 study, ZAVZPRET was statistically superior to placebo on the coprimary endpoints of pain freedom and freedom from most bothersome symptoms at two hours post-dose. The pivotal study also demonstrated pain relief as early as 15 minutes in a prespecified secondary endpoint versus placebo.
The FDA approval of ZAVZPRET marks a significant breakthrough for people with migraine who need freedom from pain and prefer alternative options to oral medications. ZAVZPRET underscores Pfizer's commitment to delivering an additional treatment option to help people with migraine regain relief and return to their daily lives.
ZAVZPRET was well tolerated in clinical trials. The most common adverse reactions reported in at least 2% of patients treated with ZAVZPRET and at a frequency greater than placebo were taste disorders (including dysgeusia and ageusia), nausea, nasal discomfort, and vomiting. ZAVZPRET is contraindicated in patients with a history of hypersensitivity to zavegepant or any of its components.
Data Bridge Market Research analyses that the migraine treatment market which was USD 2.38 billion in 2021, would rocket up to USD 4.67 billion by 2029, and is expected to undergo a CAGR of 8.80% during the forecast period 2022 to 2029. In addition to the market insights such as market value, growth rate, market segments, geographical coverage, market players, and market scenario, the market report curated by the Data Bridge Market Research team also includes in-depth expert analysis, patient epidemiology, pipeline analysis, pricing analysis, and regulatory framework.
To know more about the study, visit: https://www.databridgemarketresearch.com/reports/global-migraine-treatment-market
Challenges
Nasal sprays are a mode of drug delivery used to treat acute migraines. They offer several advantages, such as rapid onset of action and ease of use, but they also come with challenges that both patients and healthcare providers need to consider.
Nasal Delivery Addressing the Patient Needs
A 2017 study revealed that 95% of patients have at least one unmet need from their acute medication used to treat migraine. Many patients (74.1%) reported unmet needs associated with inadequate treatment response. Specifically, inadequate pain freedom at 2 h (48.1%) and headache recurrence within 24 h of initial relief (38%) were the two most common unmet needs associated with treatment. Patients (89.5%) also reported attack-related unmet needs, including the lack of rapid onset (65.3%) and headache-related disability (55.6%). A recent survey that assessed which medication attributes were of most interest to patients revealed that an ideal acute medication would be fast-acting (15–30 min) and long-lasting (12–24 h), would provide complete or near complete pain relief, could be taken at any time during the migraine, and would have few or no side effects. Patients also reported being willing to accept minor side effects as a trade-off for increased speed and efficacy. These results suggest that the current treatment approach for many migraine patients is suboptimal and may explain treatment dissatisfaction.
Although oral medications are often effective, their onset of action may be slow due to gastric stasis that may be exacerbated in a migraine attack and the rate of subsequent absorption from the small intestine, and these delays may be worse for patients with nausea or vomiting. Such symptoms, which can be bothersome, even the most bothersome, may discourage patients from taking oral medication, and once vomiting has occurred after oral medication has been taken, it may cause anxiety about whether to take a repeat dose. Administration of drugs via nasal delivery may overcome some of the limitations of oral administration, providing rapid absorption and resulting in a swift onset of action.
Nasal delivery can provide an attractive avenue to achieve the consensus goals of rapid and consistent freedom from pain. Rates of early pain relief and pain freedom favor nasal delivery over oral delivery for some triptans, with nasal delivery offering relief in as little as 15 min post-dose. Additionally, nasal delivery can result in less headache-related disability and migraine-associated symptoms compared to oral delivery. Nasal delivery offers consistency in headache response and lasting, durable relief from pain. Finally, nasal delivery provides patients with the power to decide when and where to take treatment from easy-to-use, portable devices that may allow them to take control of their disease.
Advantages of Nasal Drug Delivery
Conclusion and Future
In summary, nasal sprays have emerged as a valuable option for the acute treatment of migraines due to their rapid absorption and ability to provide timely relief from migraine symptoms. They offer an effective alternative to traditional oral medications, particularly for individuals who experience difficulties with oral intake during a migraine attack.
Nasal delivery is a well-established route of drug administration. However, most nasal sprays for the acute treatment of migraine target the lower nasal space, where absorption is limited due to quick elimination from nasal drip or clearance to the nasopharynx and rapid mucociliary clearance. Upper nasal delivery provides well-tolerated, rapid, and efficient drug absorption, and improved bioavailability compared to lower nasal delivery, ensuring quick and durable migraine relief. Delivery of drugs to the highly vascularized and absorptive upper nasal space may be an optimal route for migraine therapy. Although few products targeting the upper nasal space exist, this technology expands the possibilities of nasal drug delivery with an easy-to-use, portable device.
DBMR has served more than 40% of Fortune 500 firms internationally and has a network of more than 5000 clients. Our Team would be happy to help you with your queries. Visit, https://www.databridgemarketresearch.com/contact
Contact Us